Ways To Spot Severs Disease?
Overview
When recurring heel pain occurs in children, it is usually due to Sever's Disease, while adult heel pain is usually due to heel spurs, plantar fasciitis, or retrocalcaneal bursitis (Haglund's Deformity). Calcaneus is the anatomical name of the heel bone. Sever's Disease or Calcaneal Apophysitis is an inflammation of the growth plate located at the posterior aspect (back) of the heel.
Causes
This condition most commonly occurs due to repetitive or prolonged activities placing strain on the heel's growth plate, typically during a period of rapid growth. These activities (or sports) usually involve excessive walking, running, jumping or hopping. Severs disease may also be more likely to occur following a poorly rehabilitated sprained ankle, in patients with poor foot biomechanics or those who use inappropriate footwear. In young athletes, this condition is commonly seen in running and jumping sports, such as football, basketball, netball and athletics.
Symptoms
Sever condition causes pain at the back of the heel. The pain is increased with plantar flexion of the ankle (pushing down with the foot as if stepping on the gas), particularly against resistance. Sever condition also causes tenderness and swelling in the area of the pain.
Diagnosis
Sever's disease is based on the symptoms reported. To confirm the diagnosis, the clinician will examine the heels and ask about the child's activity level and participation in sports. They may also squeeze the back part of the heel from both sides at the same time to see if doing so causes pain and also ask the child to stand on tiptoes to see if that position causes pain. There may be tightness in the calf muscle, which contributes to tension on the heel. Symptoms are usually worse during or after activity and get better with rest. X-rays generally are not that helpful in diagnosing Sever's disease, but they may be ordered to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
If your child have Sever's disease, the following is suggested, cut back on sporting activities, don't stop, just reduce the amount until symptoms improve (if the condition has been present for a while, a total break from sport may be needed later) avoid going barefoot, a soft cushioning heel raise is really important (this reduces the pull from the calf muscles on the growth plate and increases the shock absorption, so the growth plate is not knocked around as much). Stretch the calf muscles, provided the stretch does not cause pain in the area of the growth plate). The use of an ice pack after activity for 20mins is often useful for calcaneal apophysitis - this should be repeated 2 to 3 times a day.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
When recurring heel pain occurs in children, it is usually due to Sever's Disease, while adult heel pain is usually due to heel spurs, plantar fasciitis, or retrocalcaneal bursitis (Haglund's Deformity). Calcaneus is the anatomical name of the heel bone. Sever's Disease or Calcaneal Apophysitis is an inflammation of the growth plate located at the posterior aspect (back) of the heel.
Causes
This condition most commonly occurs due to repetitive or prolonged activities placing strain on the heel's growth plate, typically during a period of rapid growth. These activities (or sports) usually involve excessive walking, running, jumping or hopping. Severs disease may also be more likely to occur following a poorly rehabilitated sprained ankle, in patients with poor foot biomechanics or those who use inappropriate footwear. In young athletes, this condition is commonly seen in running and jumping sports, such as football, basketball, netball and athletics.
Symptoms
Sever condition causes pain at the back of the heel. The pain is increased with plantar flexion of the ankle (pushing down with the foot as if stepping on the gas), particularly against resistance. Sever condition also causes tenderness and swelling in the area of the pain.
Diagnosis
Sever's disease is based on the symptoms reported. To confirm the diagnosis, the clinician will examine the heels and ask about the child's activity level and participation in sports. They may also squeeze the back part of the heel from both sides at the same time to see if doing so causes pain and also ask the child to stand on tiptoes to see if that position causes pain. There may be tightness in the calf muscle, which contributes to tension on the heel. Symptoms are usually worse during or after activity and get better with rest. X-rays generally are not that helpful in diagnosing Sever's disease, but they may be ordered to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray.
Non Surgical Treatment
If your child have Sever's disease, the following is suggested, cut back on sporting activities, don't stop, just reduce the amount until symptoms improve (if the condition has been present for a while, a total break from sport may be needed later) avoid going barefoot, a soft cushioning heel raise is really important (this reduces the pull from the calf muscles on the growth plate and increases the shock absorption, so the growth plate is not knocked around as much). Stretch the calf muscles, provided the stretch does not cause pain in the area of the growth plate). The use of an ice pack after activity for 20mins is often useful for calcaneal apophysitis - this should be repeated 2 to 3 times a day.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Tibialis Posterior Tendon Dysfunction Surgery
Overview
Adults with an acquired flatfoot deformity may present not with foot deformity but almost uniformly with medial foot pain and decreased function of the affected foot (for a list of causes of an acquired flatfoot deformity in adults. Patients whose acquired flatfoot is associated with a more generalised medical problem tend to receive their diagnosis and are referred appropriately. However, in patients whose ?adult acquired flatfoot deformity? is a result of damage to the structures supporting the medial longitudinal arch, the diagnosis is often not made early. These patients are often otherwise healthier and tend to be relatively more affected by the loss of function resulting from an acquired flatfoot deformity. The most common cause of an acquired flatfoot deformity in an otherwise healthy adult is dysfunction of the tibialis posterior tendon, and this review provides an outline to its diagnosis and treatment. 
Causes
The cause of posterior tibial tendon insufficiency is not completely understood. The condition commonly does not start from one acute trauma but is a process of gradual degeneration of the soft tissues supporting the medial (inner) side of the foot. It is most often associated with a foot that started out somewhat flat or pronated (rolled inward). This type of foot places more stress on the medial soft tissue structures, which include the posterior tibial tendon and ligaments on the inner side of the foot. Children nearly fully grown can end up with flat feet, the majority of which are no problem. However, if the deformity is severe enough it can cause significant functional limitations at that age and later on if soft tissue failure occurs. Also, young adults with normally aligned feet can acutely injure their posterior tibial tendon from a trauma and not develop deformity. The degenerative condition in patients beyond their twenties is different from the acute injuries in young patients or adolescent deformities, where progression of deformity is likely to occur.
Symptoms
Symptoms of pain may have developed gradually as result of overuse or they may be traced to one minor injury. Typically, the pain localizes to the inside (medial) aspect of the ankle, under the medial malleolus. However, some patients will also experience pain over the outside (lateral) aspect of the hindfoot because of the displacement of the calcaneus impinging with the lateral malleolus. This usually occurs later in the course of the condition. Patients may walk with a limp or in advanced cases be disabled due to pain. They may also have noticed worsening of their flatfoot deformity.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
The following is a summary of conservative treatments for acquired flatfoot. Stage 1, NSAIDs and short-leg walking cast or walker boot for 6-8 weeks; full-length semirigid custom molded orthosis, physical therapy. Stage 2, UCBL orthosis or short articulated ankle orthosis. Stage 3, Molded AFO, double-upright brace, or patellar tendon-bearing brace. Stage 4, Molded AFO, double-upright brace, or patellar tendon-bearing brace. 
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot). Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot - meaning you will be on crutches for two months. The bottom line is, Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.
What Is The Treatment And Cause Of Adult Aquired Flat Feet
Overview
Adult-Acquired Flat Foot Deformity (AAFFD) is most commonly caused by a progressive degeneration of the tendon (tibialis posterior) that supports the arch of the foot. As the tendon ages or is subjected to repetitive trauma, it stretches out over time, the natural arch of the foot becomes less pronounced and the foot gradually flattens out. Although it is uncertain why this occurs, the problem is seen equally among men and women - at an increasing frequency with age. Occasionally, a patient will experience a traumatic form of the condition as a result of a fall from a height or abnormal landing during aerial sports such as gymnastics or basketball.
Causes
There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction.
Symptoms
Symptoms shift around a bit, depending on what stage of PTTD you?re in. For instance, you?re likely to start off with tendonitis, or inflammation of the posterior tibial tendon. This will make the area around the inside of your ankle and possibly into your arch swollen, reddened, warm to the touch, and painful. Inflammation may actually last throughout the stages of PTTD. The ankle will also begin to roll towards the inside of the foot (pronate), your heel may tilt, and you may experience some pain in your leg (e.g. shin splints). As the condition progresses, the toes and foot begin to turn outward, so that when you look at your foot from the back (or have a friend look for you, because-hey-that can be kind of a difficult
maneuver to pull off) more toes than usual will be visible on the outside (i.e. the side with the pinky toe). At this stage, the foot?s still going to be flexible, although it will likely have flattened somewhat due to the lack of support from the posterior tibial tendon. You may also find it difficult to stand on your toes. Finally, you may reach a stage in which your feet are inflexibly flat. At this point, you may experience pain below your ankle on the outside of your foot, and you might even develop arthritis in the ankle.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried.

Surgical Treatment
Types of surgery your orthopaedist may discuss with you include arthrodesis, or welding (fusing) one or more of the bones in the foot/ankle together. Osteotomy, or cutting and reshaping a bone to correct alignment. Excision, or removing a bone or bone spur. Synovectomy, or cleaning the sheath covering a tendon. Tendon transfer, or using a piece of one tendon to lengthen or replace another. Having flat feet is a serious matter. If you are experiencing foot pain and think it may be related to flat feet, talk to your orthopaedist.
Adult-Acquired Flat Foot Deformity (AAFFD) is most commonly caused by a progressive degeneration of the tendon (tibialis posterior) that supports the arch of the foot. As the tendon ages or is subjected to repetitive trauma, it stretches out over time, the natural arch of the foot becomes less pronounced and the foot gradually flattens out. Although it is uncertain why this occurs, the problem is seen equally among men and women - at an increasing frequency with age. Occasionally, a patient will experience a traumatic form of the condition as a result of a fall from a height or abnormal landing during aerial sports such as gymnastics or basketball.
Causes
There are numerous causes of acquired adult flatfoot, including fracture or dislocation, tendon laceration, tarsal coalition, arthritis, neuroarthropathy, neurologic weakness, and iatrogenic causes. The most common cause of acquired adult flatfoot is posterior tibial tendon dysfunction.
Symptoms
Symptoms shift around a bit, depending on what stage of PTTD you?re in. For instance, you?re likely to start off with tendonitis, or inflammation of the posterior tibial tendon. This will make the area around the inside of your ankle and possibly into your arch swollen, reddened, warm to the touch, and painful. Inflammation may actually last throughout the stages of PTTD. The ankle will also begin to roll towards the inside of the foot (pronate), your heel may tilt, and you may experience some pain in your leg (e.g. shin splints). As the condition progresses, the toes and foot begin to turn outward, so that when you look at your foot from the back (or have a friend look for you, because-hey-that can be kind of a difficult
maneuver to pull off) more toes than usual will be visible on the outside (i.e. the side with the pinky toe). At this stage, the foot?s still going to be flexible, although it will likely have flattened somewhat due to the lack of support from the posterior tibial tendon. You may also find it difficult to stand on your toes. Finally, you may reach a stage in which your feet are inflexibly flat. At this point, you may experience pain below your ankle on the outside of your foot, and you might even develop arthritis in the ankle.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
A patient who has acute tenosynovitis has pain and swelling along the medial aspect of the ankle. The patient is able to perform a single-limb heel-rise test but has pain when doing so. Inversion of the foot against resistance is painful but still strong. The patient should be managed with rest, the administration of appropriate anti-inflammatory medication, and immobilization. The injection of corticosteroids is not recommended. Immobilization with either a rigid below-the-knee cast or a removable cast or boot may be used to prevent overuse and subsequent rupture of the tendon. A removable stirrup-brace is not initially sufficient as it does not limit motion in the sagittal plane, a component of the pathological process. The patient should be permitted to walk while wearing the cast or boot during the six to eight-week period of immobilization. At the end of that time, a decision must be made regarding the need for additional treatment. If there has been marked improvement, the patient may begin wearing a stiff-soled shoe with a medial heel-and-sole wedge to invert the hindfoot. If there has been only mild or moderate improvement, a longer period in the cast or boot may be tried.
Surgical Treatment
Types of surgery your orthopaedist may discuss with you include arthrodesis, or welding (fusing) one or more of the bones in the foot/ankle together. Osteotomy, or cutting and reshaping a bone to correct alignment. Excision, or removing a bone or bone spur. Synovectomy, or cleaning the sheath covering a tendon. Tendon transfer, or using a piece of one tendon to lengthen or replace another. Having flat feet is a serious matter. If you are experiencing foot pain and think it may be related to flat feet, talk to your orthopaedist.
Adult Aquired FlatFoot
Overview
Posterior tibial tendon insufficiency (also called posterior tibial tendon dysfunction or adult acquired flatfoot) has been named literally after failure of the posterior tibial tendon. However, the condition is caused not only by the progressive failure of the posterior tibial tendon; it is also failure of associated ligaments and joints on the inner side of the ankle and foot. This results in collapse of the arch of the foot, along with the deformity which most often becomes the debilitating problem in its later stages. While at the beginning the common symptom is pain over the tendon in the inner part of the hindfoot and midfoot, later on it is the deformity that can threaten a person's ability to walk. Just as the tendon degenerates and loses its function, other soft tissue on the same inner side of the foot - namely the ligaments - degenerate and fail. Ligaments are responsible for holding bones in place, and when they fail, bones shift to places where they shouldn?t; deformity is the result. The deformity causes malalignment, leading to more stress and failure of the ligaments.
Causes
Rheumatoid arthritis This type of arthritis attacks the cartilage in the foot, leading to pain and flat feet. It is caused by auto-immune disease, where the body?s immune system attacks its own tissues. Diabetes. Having diabetes can cause nerve damage and affect the feeling in your feet and cause arch collapse. Bones can also fracture but some patients may not feel any pain due to the nerve damage. Obesity and/or hypertension (high blood pressure) This increases your risk of tendon damage and resulting flat foot.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. Asymmetrical collapsing of the medial arch on the affected side.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
The adult acquired flatfoot is best treated early. There is no recommended home treatment other than the general avoidance of prolonged weightbearing in non-supportive footwear until the patient can be seen in the office of the foot and ankle specialist. In Stage I, the inflammation and tendon injury will respond to rest, protected ambulation in a cast, as well as anti-inflammatory therapy. Follow-up treatment with custom-molded foot orthoses and properly designed athletic or orthopedic footwear are critical to maintain stability of the foot and ankle after initial symptoms have been calmed. Once the tendon has been stretched, the foot will become deformed and visibly rolled into a pronated position at the ankle. Non-surgical treatment has a significantly lower chance of success. Total immobilization in a cast or Camwalker may calm down symptoms and arrest progression of the deformity in a smaller percentage of patients. Usually, long-term use of a brace known as an ankle foot orthosis is required to stop progression of the deformity without surgery. A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.

Surgical Treatment
Until recently, operative treatment was indicated for most patients with stage 2 deformities. However, with the use of potentially effective nonoperative management , operative treatment is now indicated for those patients that have failed nonoperative management. The principles of operative treatment of stage 2 deformities include transferring another tendon to help serve the role of the dysfunctional posterior tibial tendon (usually the flexor hallucis longus is transferred). Restoring the shape and alignment of the foot. This moves the weight bearing axis back to the center of the ankle. Changing the shape of the foot can be achieved by one or more of the following procedures. Cutting the heel bone and shifting it to the inside (Medializing calcaneal osteotomy). Lateral column lengthening restores the arch and overall alignment of the foot. Medial column stabilization. This stiffens the ray of the big toe to better support the arch. Lengthening of the Achilles tendon or Gastrocnemius. This will allow the ankle to move adequately once the alignment of the foot is corrected. Stage 3 acquired adult flatfoot deformity is treated operatively with a hindfoot fusion (arthrodesis). This is done with either a double or triple arthrodesis - fusion of two or three of the joints in hindfoot through which the deformity occurs. It is important when a hindfoot arthrodesis is performed that it be done in such a way that the underlying foot deformity is corrected first. Simply fusing the hindfoot joints in place is no longer acceptable.
Posterior tibial tendon insufficiency (also called posterior tibial tendon dysfunction or adult acquired flatfoot) has been named literally after failure of the posterior tibial tendon. However, the condition is caused not only by the progressive failure of the posterior tibial tendon; it is also failure of associated ligaments and joints on the inner side of the ankle and foot. This results in collapse of the arch of the foot, along with the deformity which most often becomes the debilitating problem in its later stages. While at the beginning the common symptom is pain over the tendon in the inner part of the hindfoot and midfoot, later on it is the deformity that can threaten a person's ability to walk. Just as the tendon degenerates and loses its function, other soft tissue on the same inner side of the foot - namely the ligaments - degenerate and fail. Ligaments are responsible for holding bones in place, and when they fail, bones shift to places where they shouldn?t; deformity is the result. The deformity causes malalignment, leading to more stress and failure of the ligaments.
Causes
Rheumatoid arthritis This type of arthritis attacks the cartilage in the foot, leading to pain and flat feet. It is caused by auto-immune disease, where the body?s immune system attacks its own tissues. Diabetes. Having diabetes can cause nerve damage and affect the feeling in your feet and cause arch collapse. Bones can also fracture but some patients may not feel any pain due to the nerve damage. Obesity and/or hypertension (high blood pressure) This increases your risk of tendon damage and resulting flat foot.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. Asymmetrical collapsing of the medial arch on the affected side.
Diagnosis
The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is.
Non surgical Treatment
The adult acquired flatfoot is best treated early. There is no recommended home treatment other than the general avoidance of prolonged weightbearing in non-supportive footwear until the patient can be seen in the office of the foot and ankle specialist. In Stage I, the inflammation and tendon injury will respond to rest, protected ambulation in a cast, as well as anti-inflammatory therapy. Follow-up treatment with custom-molded foot orthoses and properly designed athletic or orthopedic footwear are critical to maintain stability of the foot and ankle after initial symptoms have been calmed. Once the tendon has been stretched, the foot will become deformed and visibly rolled into a pronated position at the ankle. Non-surgical treatment has a significantly lower chance of success. Total immobilization in a cast or Camwalker may calm down symptoms and arrest progression of the deformity in a smaller percentage of patients. Usually, long-term use of a brace known as an ankle foot orthosis is required to stop progression of the deformity without surgery. A new ankle foot orthosis known as the Richie Brace, offered by PAL Health Systems, has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.
Surgical Treatment
Until recently, operative treatment was indicated for most patients with stage 2 deformities. However, with the use of potentially effective nonoperative management , operative treatment is now indicated for those patients that have failed nonoperative management. The principles of operative treatment of stage 2 deformities include transferring another tendon to help serve the role of the dysfunctional posterior tibial tendon (usually the flexor hallucis longus is transferred). Restoring the shape and alignment of the foot. This moves the weight bearing axis back to the center of the ankle. Changing the shape of the foot can be achieved by one or more of the following procedures. Cutting the heel bone and shifting it to the inside (Medializing calcaneal osteotomy). Lateral column lengthening restores the arch and overall alignment of the foot. Medial column stabilization. This stiffens the ray of the big toe to better support the arch. Lengthening of the Achilles tendon or Gastrocnemius. This will allow the ankle to move adequately once the alignment of the foot is corrected. Stage 3 acquired adult flatfoot deformity is treated operatively with a hindfoot fusion (arthrodesis). This is done with either a double or triple arthrodesis - fusion of two or three of the joints in hindfoot through which the deformity occurs. It is important when a hindfoot arthrodesis is performed that it be done in such a way that the underlying foot deformity is corrected first. Simply fusing the hindfoot joints in place is no longer acceptable.
Achilles Tendonitis Pain
Overview
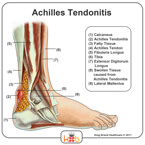
 The Achilles tendon is the tendon that attaches the gastrocnemius (calf muscles) to the calcaneus bone (back of the heel). It is important in activities that involve plantar flexion of the ankle (pushing down with the foot or doing heel raises). The Achilles tendon can get inflamed (tendinitis) or it can degenerate/wear out (tendinopathy) with repetitive activities. Aggravating activities include running and/or repetitive jumping.
The Achilles tendon is the tendon that attaches the gastrocnemius (calf muscles) to the calcaneus bone (back of the heel). It is important in activities that involve plantar flexion of the ankle (pushing down with the foot or doing heel raises). The Achilles tendon can get inflamed (tendinitis) or it can degenerate/wear out (tendinopathy) with repetitive activities. Aggravating activities include running and/or repetitive jumping.
Causes
Some of the causes of Achilles tendonitis include, overuse injury - this occurs when the Achilles tendon is stressed until it develops small tears. Runners seem to be the most susceptible. People who play sports that involve jumping, such as basketball, are also at increased risk. Arthritis - Achilles tendonitis can be a part of generalised inflammatory arthritis, such as ankylosing spondylitis or psoriatic arthritis. In these conditions, both tendons can be affected. Foot problems - some people with flat feet or hyperpronated feet (feet that turn inward while walking) are prone to Achilles tendonitis. The flattened arch pulls on calf muscles and keeps the Achilles tendon under tight strain. This constant mechanical stress on the heel and tendon can cause inflammation, pain and swelling of the tendon. Being overweight can make the problem worse. Footwear - wearing shoes with minimal support while walking or running can increase the risk, as can wearing high heels. Overweight and obesity - being overweight places more strain on many parts of the body, including the Achilles tendon. Quinolone antibiotics - can in some instances be associated with inflammatory tenosynovitis and, if present, will often be bilateral (both Achilles), coming on soon after exposure to the drug.
Symptoms
The main complaint associated with Achilles tendonitis is pain behind the heel. The pain is often most prominent in an area about 2-4 centimeters above where the tendon attaches to the heel. In this location, called the watershed zone of the tendon, the blood supply to the tendon makes this area particularly susceptible. Patients with Achilles tendonitis usually experience the most significant pain after periods of inactivity. Therefore patients tend to experience pain after first walking in the morning and when getting up after sitting for long periods of time. Patients will also experience pain while participating in activities, such as when running or jumping. Achilles tendonitis pain associated with exercise is most significant when pushing off or jumping.
Diagnosis
To diagnose the condition correctly, your doctor will ask you a few questions about the pain and swelling in your heel. You may be asked to stand on the balls of your feet while your doctor observes your range of motion and flexibility. The doctor may also touch the area directly. This allows him to pinpoint where the pain and swelling is most severe.
Nonsurgical Treatment
Treatment approaches for Achilles tendonitis or tendonosis are selected on the basis of how long the injury has been present and the degree of damage to the tendon. In the early stage, when there is sudden (acute) inflammation, one or more of the following options may be recommended. Immobilization. Immobilization may involve the use of a cast or removable walking boot to reduce forces through the Achilles tendon and promote healing. Ice. To reduce swelling due to inflammation, apply a bag of ice over a thin towel to the affected area for 20 minutes of each waking hour. Do not put ice directly against the skin. Oral medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be helpful in reducing the pain and inflammation in the early stage of the condition. Orthotics. For those with over-pronation or gait abnormalities, custom orthotic devices may be prescribed. Night splints. Night splints help to maintain a stretch in the Achilles tendon during sleep. Physical therapy. Physical therapy may include strengthening exercises, soft-tissue massage/mobilization, gait and running re-education, stretching, and ultrasound therapy.
Surgical Treatment
There are three common procedures that doctor preform in order help heal the tendinitis depending on the location of the tendinitis and amount of damage to the tendon, including: Gastrocnemius recession - With this surgery doctors lengthen the calf muscles because the tight muscles increases stress on the Achilles tendon. The procedure is typically done on people who have difficulty flexing their feet even with constant stretching. Debridement and Repair - When there is less than 50% damage in the tendon, it is possible for doctors to remove the injured parts and repair the healthy portions. This surgery is most done for patients who are suffering from bone spurs or arthritis. To repair the tendon doctors may use metal or plastic anchors to help hold the Achilles tendon in place. Patients have to wear a boot or cast for 2 weeks or more, depending and the damage done to the tendon. Debridement with Tendon Transfer - When there is more the 50% damage done to the Achilles tendon, and Achilles tendon transfer is preformed because the remain healthy tissue is not strong enough. The tendon that helps the big toe move is attached to give added strength to the damaged Achilles. After surgery, most patients don?t notice any difference when they walk or run.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
The Achilles tendon is the tendon that attaches the gastrocnemius (calf muscles) to the calcaneus bone (back of the heel). It is important in activities that involve plantar flexion of the ankle (pushing down with the foot or doing heel raises). The Achilles tendon can get inflamed (tendinitis) or it can degenerate/wear out (tendinopathy) with repetitive activities. Aggravating activities include running and/or repetitive jumping.
Causes
Some of the causes of Achilles tendonitis include, overuse injury - this occurs when the Achilles tendon is stressed until it develops small tears. Runners seem to be the most susceptible. People who play sports that involve jumping, such as basketball, are also at increased risk. Arthritis - Achilles tendonitis can be a part of generalised inflammatory arthritis, such as ankylosing spondylitis or psoriatic arthritis. In these conditions, both tendons can be affected. Foot problems - some people with flat feet or hyperpronated feet (feet that turn inward while walking) are prone to Achilles tendonitis. The flattened arch pulls on calf muscles and keeps the Achilles tendon under tight strain. This constant mechanical stress on the heel and tendon can cause inflammation, pain and swelling of the tendon. Being overweight can make the problem worse. Footwear - wearing shoes with minimal support while walking or running can increase the risk, as can wearing high heels. Overweight and obesity - being overweight places more strain on many parts of the body, including the Achilles tendon. Quinolone antibiotics - can in some instances be associated with inflammatory tenosynovitis and, if present, will often be bilateral (both Achilles), coming on soon after exposure to the drug.
Symptoms
The main complaint associated with Achilles tendonitis is pain behind the heel. The pain is often most prominent in an area about 2-4 centimeters above where the tendon attaches to the heel. In this location, called the watershed zone of the tendon, the blood supply to the tendon makes this area particularly susceptible. Patients with Achilles tendonitis usually experience the most significant pain after periods of inactivity. Therefore patients tend to experience pain after first walking in the morning and when getting up after sitting for long periods of time. Patients will also experience pain while participating in activities, such as when running or jumping. Achilles tendonitis pain associated with exercise is most significant when pushing off or jumping.
Diagnosis
To diagnose the condition correctly, your doctor will ask you a few questions about the pain and swelling in your heel. You may be asked to stand on the balls of your feet while your doctor observes your range of motion and flexibility. The doctor may also touch the area directly. This allows him to pinpoint where the pain and swelling is most severe.
Nonsurgical Treatment
Treatment approaches for Achilles tendonitis or tendonosis are selected on the basis of how long the injury has been present and the degree of damage to the tendon. In the early stage, when there is sudden (acute) inflammation, one or more of the following options may be recommended. Immobilization. Immobilization may involve the use of a cast or removable walking boot to reduce forces through the Achilles tendon and promote healing. Ice. To reduce swelling due to inflammation, apply a bag of ice over a thin towel to the affected area for 20 minutes of each waking hour. Do not put ice directly against the skin. Oral medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be helpful in reducing the pain and inflammation in the early stage of the condition. Orthotics. For those with over-pronation or gait abnormalities, custom orthotic devices may be prescribed. Night splints. Night splints help to maintain a stretch in the Achilles tendon during sleep. Physical therapy. Physical therapy may include strengthening exercises, soft-tissue massage/mobilization, gait and running re-education, stretching, and ultrasound therapy.
Surgical Treatment
There are three common procedures that doctor preform in order help heal the tendinitis depending on the location of the tendinitis and amount of damage to the tendon, including: Gastrocnemius recession - With this surgery doctors lengthen the calf muscles because the tight muscles increases stress on the Achilles tendon. The procedure is typically done on people who have difficulty flexing their feet even with constant stretching. Debridement and Repair - When there is less than 50% damage in the tendon, it is possible for doctors to remove the injured parts and repair the healthy portions. This surgery is most done for patients who are suffering from bone spurs or arthritis. To repair the tendon doctors may use metal or plastic anchors to help hold the Achilles tendon in place. Patients have to wear a boot or cast for 2 weeks or more, depending and the damage done to the tendon. Debridement with Tendon Transfer - When there is more the 50% damage done to the Achilles tendon, and Achilles tendon transfer is preformed because the remain healthy tissue is not strong enough. The tendon that helps the big toe move is attached to give added strength to the damaged Achilles. After surgery, most patients don?t notice any difference when they walk or run.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
What Is Pain In The Heel And Ideas On How To Treat It

Overview
The American College of Sports and Medicine (1) estimates that the average adult takes between 5,000 and 10,000 steps per day. The brunt of this activity is borne by the bones, muscles and ligaments of the foot. Healthy feet have strong, wonderfully flexible ligaments which are designed to support standing, walking and running. Plantar Fasciitis (pronounced "plantar fash-ee-eye-tis") is defined as inflammation of, or damage to, one of the most important ligaments in the foot - the plantar fascia. The plantar fascia ligament is located along the sole of your foot. It is made up of fibrous tissue that stretches outward from the heel bone, like a strong piece of elastic, and then branches out across the arch and through the ball area of the foot toward the toes.
Causes
As a person gets older, the plantar fascia becomes less like a rubber band and more like a rope that doesn't stretch very well. The fat pad on the heel becomes thinner and can't absorb as much of the shock caused by walking. The extra shock damages the plantar fascia and may cause it to swell, tear or bruise. You may notice a bruise or swelling on your heel. Other risk factors for plantar fasciitis include being overweight and obesity. Diabetes. Spending most of the day on your feet. Becoming very active in a short period of time. Being flat-footed or having a high arch.
Symptoms
If you have Plantar Fasciitis, you will most likely feel a sharp pain under the ball of you heel and it will often give pain when standing after a period of rest. For example when you get out of bed in the mornings or after being sat down. Some patients describe this feeling as a stone bruise sensation, or a pebble in the shoe and at times the pain can be excruciating. Patients with Plantar Fasciitis can experience pain free periods whereby the think they are on the mend, only for the heel pain to come back aggressively when they appear to have done nothing wrong. If your plantar fasciitis came on very suddenly and the pain is relentless, then you may have Plantar Fascial Tears. We will be able to differentiate between these 2 conditions, sometimes with ultra sound imaging. The treatment for each of these conditions will need to be very different.
Diagnosis
A physical exam performed in the office along with the diagnostic studies as an x-ray. An MRI may also be required to rule out a stress fracture, or a tear of the plantar fascia. These are conditions that do not normally respond to common plantar fasciitis treatment.
Non Surgical Treatment
No single treatment works best for everyone with plantar fasciitis. But there are many things you can try to help your foot get better. Give your feet a rest. Cut back on activities that make your foot hurt. Try not to walk or run on hard surfaces. To reduce pain and swelling, try putting ice on your heel. Or take an over-the-counter pain reliever like ibuprofen (such as Advil or Motrin) or naproxen (such as Aleve). Do toe stretches , calf stretches and towel stretches several times a day, especially when you first get up in the morning. (For towel stretches, you pull on both ends of a rolled towel that you place under the ball of your foot.) Get a new pair of shoes. Pick shoes with good arch support and a cushioned sole. Or try heel cups or shoe inserts ( orthotics ). Use them in both shoes, even if only one foot hurts. If these treatments do not help, your doctor may recommend splints that you wear at night, shots of medicine (such as a steroid ) in your heel, or other treatments. You probably will not need surgery. Doctors only suggest it for people who still have pain after trying other treatments for 6 to 12 months.

Surgical Treatment
Most studies indicate that 95% of those afflicted with plantar fasciitis are able to relieve their heel pain with nonsurgical treatments. If you are one of the few people whose symptoms don't improve with other treatments, your doctor may recommend plantar fascia release surgery. Plantar fascia release involves cutting part of the plantar fascia ligament in order to release the tension and relieve the inflammation of the ligament. Overall, the success rate of surgical release is 70 to 90 percent in patients with plantar fasciitis. While the success rate is very high following surgery, one should be aware that there is often a prolonged postoperative period of discomfort similar to the discomfort experienced prior to surgery. This pain usually will abate within 2-3 months. One should always be sure to understand all the risks associated with any surgery they are considering.
What Leads To Pain Of The Heel To Appear

Overview
Plantar fasciitis is a dull to severe pain in your heel caused by a strain and inflammation of your plantar fascia. The plantar fascia is a scientific name for “foot tissue”. This particular tissue is a ligament attached at one side to the heel bone. At the other side, the tissue fans out to attach at the base of each of your five toes. Plantar fasciitis is the name for the condition that develops when that tissue becomes inflamed. When the plantar fascia is excessively stretched, micro-tears can occur, causing this swelling and subsequent pain.
Causes
Training on improper, hard and/or irregular surfaces as well as excessive track work in spiked shoes, or steep hill running, can stress the plantar fascia past its limits of elasticity, leading to injury. Finally, failure in the early season to warm up gradually gives the athlete insufficient time for the structures of the foot to re-acclimate and return to a proper fitness level for intensive exercise. Such unprepared and repeated trauma causes microscopic tearing, which may only be detected once full-blown plantar fasciitis and accompanying pain and debilitation have resulted. If the level of damage to the plantar fascia is significant, an inflammatory reaction of the heel bone can produce spike-like projections of new bone, known as heel spurs. Indeed, plantar fasciitis has occasionally been refereed to as heel spur syndrome, though such spurs are not the cause of the initial pain but are instead a further symptom of the problem. While such spurs are sometimes painless, in other cases they cause pain or disability in the athlete, and surgical intervention to remove them may be required. A dull, intermittent pain in the heel is typical, sometimes progressing to a sharp, sustained discomfort. Commonly, pain is worse in the morning or after sitting, later decreasing as the patient begins walking, though standing or walking for long periods usually brings renewal of the pain.
Symptoms
Among the symptoms for Plantar Fasciitis is pain usually felt on the underside of the heel, often most intense with the first steps after getting out of bed in the morning. It is commonly associated with long periods of weight bearing or sudden changes in weight bearing or activity. Plantar Fasciitis also called “policeman’s heel” is presented by a sharp stabbing pain at the bottom or front of the heel bone. In most cases, heel pain is more severe following periods of inactivity when getting up and then subsides, turning into a dull ache.
Diagnosis
During the physical exam, your doctor checks for points of tenderness in your foot. The location of your pain can help determine its cause. Usually no tests are necessary. The diagnosis is made based on the history and physical examination. Occasionally your doctor may suggest an X-ray or magnetic resonance imaging (MRI) to make sure your pain isn't being caused by another problem, such as a stress fracture or a pinched nerve. Sometimes an X-ray shows a spur of bone projecting forward from the heel bone. In the past, these bone spurs were often blamed for heel pain and removed surgically. But many people who have bone spurs on their heels have no heel pain.
Non Surgical Treatment
Plantar fasciitis can be a difficult problem to treat, with no panacea available. Fortunately, most patients with this condition eventually have satisfactory outcomes with nonsurgical treatment. Therefore, management of patient expectations minimizes frustration for both the patient and the provider.

Surgical Treatment
Most patients have good results from surgery. However, because surgery can result in chronic pain and dissatisfaction, it is recommended only after all nonsurgical measures have been exhausted. The most common complications of release surgery include incomplete relief of pain and nerve damage.
Prevention
Factors that help prevent plantar fasciitis and reduce the risk of recurrence include. Exercises to strengthen the muscles of the lower leg and ankle. Warming up before commencing physical activity. Maintaining a healthy body weight. Avoiding high heeled footwear. Using orthotic devices such as arch supports and heel raises in footwear, particularly for people with very high arches or flat feet. Daily stretches of plantar fascia and Achilles tendon.